Medicine Notes Medicine and Surgery Pack Notes
Orthopaedics Notes
Updated Orthopaedics Notes

Medicine and Surgery Pack
These detailed and colour coded medical notes encompass a wide range of specialities, from Gastroenterology to Paediatrics, and is fantastic value for money.
EVERY section of notes follows the same template, so is very easy to follow, with each condition being split up as follows:
1. Summary points
2. Aetiology and pathophysiology
3. Epidemiology and associated risk factors
4. Presentation
5. Assessment - examination findings and relevant investigations
6. Management
7. Prognosis and co...
The following is a more accessible plain text extract of the PDF sample above, taken from our Medicine and Surgery Pack Notes. Due to the challenges of extracting text from PDFs, it will have odd formatting:
ORTHOPAEDICS
Contents:
Gout
Psoriatic arthritis
Psuedogout
Rheumatoid arthritis
To view pictures, just hit the link!
GOUT
Summary Points
Gout is caused by the deposition of monosodium urate crystals in a joint
Patients present with acute, severely painful, swollen joint
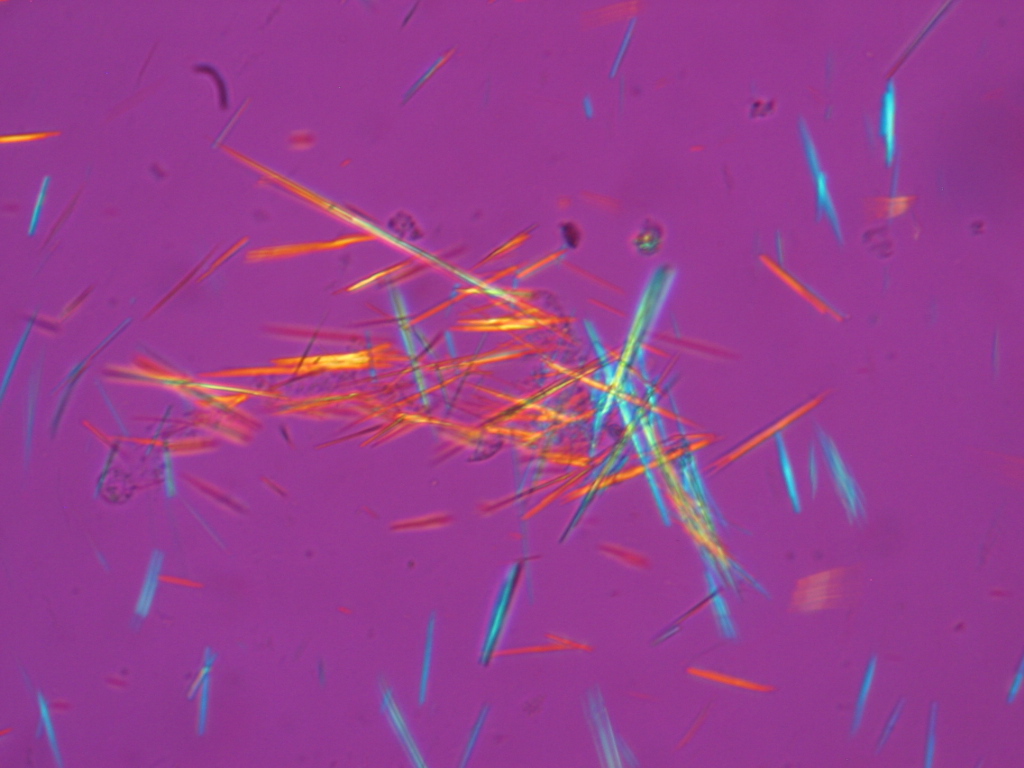
Confirm with synovial fluid aspiration, as gout crystals are negatively birefringent under polarised light
Manage acute attacks with NSAIDs, and allopurinol for prophylaxis from future attacks
Aetiology and Pathophysiology
Gout is a condition whereby there is deposition of monosodium urate monohydrate crystals in joints causing inflammation and eventual tissue damage. It is one of the most acutely painful conditions known. They affect the joints of the upper and lower limbs.
Types:
Primary 95% - acute attacks, genetic influence due to overproduction or underexcretion of uric acid
Secondary 5% - usually due to chronic diuretic therapy/changes in uric acid metabolism
Further subdivided into:
Asymptomatic
Hyperuricaemic
Acute
Intercritical/chronic tophaceous
Most patients with hyperuricaemia never develop gout and patients with gout do not need to have hyperuricaemia at the time of presentation. Crystals deposited in and around joint and can be found in synovial fluid
Most cases are due to the undersecretion of uric acid. <10% are due to its overproduction. However, important to note that you can have normoproduction w/ gout, so associated risk factors play a significant role.
Epidemiology and Associated Risk Factors
Incidence 12-18/100,000
Asian and Pacific Islanders have a much higher prevalence and a more severe disease.
Risk factors:
Male sex (5:1) - female prevalence increases after menopause
Meat and seafood
Alcohol
Obesity, high triglycerides, hypertension, coronary heart disease
Diabetes mellitus
Chronic kidney disease
Asian ethnicity
Drugs – chemotherapy, diuretics
Trauma and joint morbidity
Leukaemia
Presentation
Classically, gout presents as an acutely painful joint which is swollen, tender and erythematous, reaching a crescendo over 6-12hrs. Inflammation peaks within 24hrs, often with fever and malaise.
50% all attacks and 70% of first attacks affect the first metatarsophalangeal joint. Other sites: knee, midtarsal, wrist, ankle, small hand joints, elbows
Attacks are often spontaneous but may be triggered by trauma, surgery, alcohol consumption, starvation, infection or exercise.
Other atypical presentations:
Tenosynovitis
Bursitis
Cellulitis
Sore eyes - as the crystals can deposit in the conjunctiva
If chronic tophacecous gout, there may be irregular firm nodules (mainly around extensor surfaces of fingers, hands, forearms, elbows, Achilles tendon and ear) which are typically asymmetrical with a chalky appearance beneath the skin. Some only present with connective tissue tophi. Less often, patients present with painful tophaceous deposits and discharge in Heberden's (distal IP) and Bouchard's nodes (proximal IP).
Assessment
- O/E –
Synovitis, swelling and extreme tenderness w/ overlying erythema
Pyrexia
Restricted movement, crepitus and deformity.
Tophi (irregular firm nodules, where the monosodium urate crystals have deposited)
Heberden’s or Bouchard’s nodes, that may discharge
Picture links:
http://upload.wikimedia.org/wikipedia/commons/2/28/Gout2010.JPG
http://upload.wikimedia.org/wikipedia/commons/0/0e/ChronicGout.jpg
{kind=link}
{kind=link}
- Ix –
Must differentiate from psuedogout by inspecting crystals under polarised light
Synovial fluid aspirate -Gout crystals arenegativelybirefringent. It may require repeating if no crystals found.
Picture link: http://upload.wikimedia.org/wikipedia/commons/a/ac/Fluorescent_uric_acid.JPG
{kind=link}
Blood -
Serum uric acid levels - establishes risk but not useful diagnostic aid. >360 = raised. Uric acid levels may fall during an acute attack
Glucose to rule out DM
Lipids - associated w/ metabolic syndrome
Urine - 24hr urine sampling - renal uric acid secretion, useful for families
Imaging -
XR - soft tissue swelling in early stages, later can see punched out erosions in juxta-articular bone. Joint space preserved until late.
Rx
The objective is to alleviate pain and inflammation.
Conservative
Resolves spontaneously in 5-15 days untreated with itching and desquamation of the overlying skin.
Rest + Ice + Elevate
Fluid therapy
Advise - lose weight, exercise, diet, reduce alcohol intake and increase fluid intake
Medical
In an acute attack:
NSAIDs first line - none specified but naproxen, diclofenac or indometacin are generally preferred. May be contraindicated for peptic ulcer disease, heart failure and if on anti-coagulants.
Colchicine (an alkaloid with an unknown mechanism) is used when NSAIDs are contraindicated (or may be preferred by the individual) and is first line w/ NSAIDS according to European League Against Rheumatism. Start colchicine on 1mg increasing by 0.5mg every 2hrs until toxicity develops (nausea, diarrhoea and vomiting), the max dose being 6mg.
Steroids if NSAIDs and colchicines are contraindicated (e.g. in renal impairment). There are many ways of administration these steroids - PO, IM, IV or intra-articular.
Prophylaxis: (If have >1 attack/yr think about prophylaxis)
-
Allopurinol (xanthine oxidase inhibitor -> reduces uric acid synthesis) is first-line but never start it during an acute attack as it worsens the problem (wait 3 weeks).
Should start NSAIDs/colchicine/steroids with it for 1-3 months.
Start 50-100mg and increase (typically to 200mg) until serum uric acid <300. Max dose 900mg.
Do not stop allopurinol in a new acute attack
Allopurinol is not indicated for use in hyperuricaemic gout
Possible side effects include a rash, fever and leucopenia
Alternatives (that increase urinary excretion of uric acid):
Sulfinpyrazone - if allopurinol toxicity occurs
Probenecid
Febuxostat - recommended by NICE if allopurinol intolerant, or if it is contra-indicated
Prognosis and Complications
Complications:
Can lead to...
Buy the full version of these notes or essay plans and more in our Medicine and Surgery Pack Notes.
Orthopaedics
These detailed and colour coded medical notes encompass a wide range of specialities, from Gastroenterology to Paediatrics, and is fantastic value for money.
EVERY section of notes follows the same template, so is very easy to follow, with each condition being split up as follows:
1. Summary points
2. Aetiology and pathophysiology
3. Epidemiology and associated risk factors
4. Presentation
5. Assessment - examination findings and relevant investigations
6. Management
7. Prognosis and co...
Need instant answers? Our AI exam tutor is here to help.
Ask questions 🙋 Get answers 📔 It's simple 👁️👄👁️
Our AI is educated by the highest scoring students across all subjects and schools. Join hundreds of your peers today.
Get Started